Lifeguard’s Guide to Spotting a Stroke

Differentiating a heat emergency compared to a brain attack is a critical first responder’s responsibility.
When a patron stumbles on the beach or starts slurring their words, it’s easy to blame the harsh summer elements. On a 90-degree day, our brains automatically jump to heat exhaustion, sun glare, or severe dehydration.
But misattributing these symptoms can be a fatal mistake.
A stroke is an acute "brain attack" caused by an interrupted blood supply (ischemic) or a ruptured blood vessel (hemorrhagic) within the brain. On the beach, early stroke symptoms are frequently missed, dangerously delaying definitive medical care. When the clinical clock is ticking, ocean rescue professionals must be ready to act instantly.
Here is how to recognize a neurological emergency on your beach and what to do the moment you find one.
The HOW:
Execute the "BE FAST" Assessment
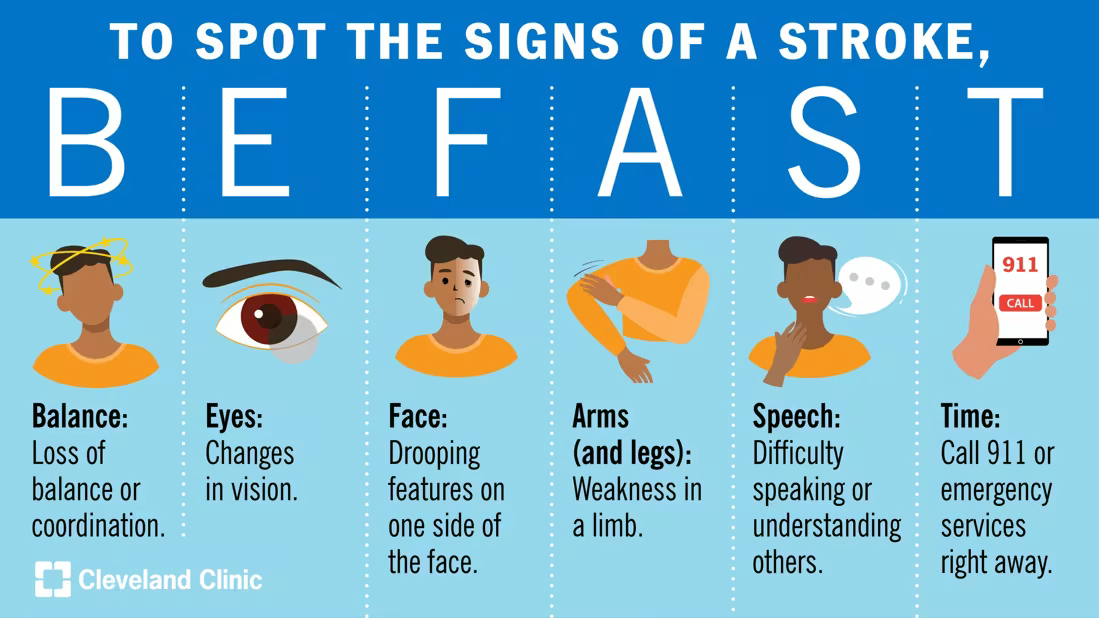
Spotting the signs of STROKE.
If you suspect a neurological deficit in a patron, do not wait. Immediately execute this six-part assessment:
B – Balance: Check for a sudden loss of balance, coordination, or unexplained dizziness. Ask the patient if they feel a sudden room-spinning sensation (vertigo) or if they are leaning severely to one side while trying to sit or stand on the sand.
E – Eyes: Assess for sudden vision changes. Are they experiencing blurred vision, double vision, or a sudden loss of sight? Check if their pupils are unequal or if their eyes are locked, gazing toward one specific side.
F – Facial Droop: Ask the patron to show their teeth or smile. Look for asymmetry—does one side of the face lag, flatten, or droop?
A – Arm Drift: Have the patient extend both arms straight out in front of them with palms up and eyes closed for 10 seconds. Watch to see if one arm automatically drifts downward or pronates (turns palm down).
S – Speech Difficulty: Ask the patient to repeat a simple, familiar phrase (e.g., "Red sky at night is a sailor’s delight"). Listen closely for slurred speech, garbled words, or an absolute inability to understand or execute the command.
T – Time: If the patient fails even a single metric of this test, activate EMS immediately. Note the exact Last Known Well (LKW) time—this governs the hospital's window for lifesaving clot-busting therapy.
The Next Steps:
Shifting from Assessor to Lifeline
Once your BE FAST assessment reveals even a single positive marker, your role shifts. You are now a high-priority conduit for Advanced Life Support. Take these actions immediately:
1. Trigger a "Stroke Alert"
Activate EMS through your organizational escalation chain using this specific phrase and “trigger words”:
"We have a confirmed positive stroke assessment using BE FAST."
Provide the patient’s exact Last Known Well (LKW) time. This triggers a "Stroke Alert" across the EMS chain, ensuring the responding ambulance is routed to a certified Stroke Center and specialized neurological teams are spun up before the patient arrives.
2. Manage Body Positioning (The 30-Degree Rule)
Conscious Patient: Do not lay a stroke patient completely flat, as intracranial pressure (swelling in the brain) can increase. Do not sit them up too high, or blood pressure to the brain can drop. Place the victim in a shaded area, elevating their head and torso to roughly 30 degrees.
Unresponsive/Vomiting Patient: Place them immediately into the Recovery Position on their left side to protect the airway, keeping the neck straight.
3. Absolute NPO (Nothing by Mouth)
Strokes frequently paralyze the muscles responsible for swallowing (dysphagia). Do not give the victim anything to eat or drink. Giving a stroke patient water, aspirin, or oral glucose can lead to immediate aspiration into the lungs, triggering respiratory failure. If they complain of a dry mouth, use a damp gauze pad to gently moisten their lips, but do not allow them to swallow fluid.
4. Gather Critical Data for Paramedics
While transport teams cross the sand, secure this vital information from family or friends:
The LKW Time: Exactly what time was the patient last seen normal - “last known well” time?
Blood Thinners: Is the patient taking any anticoagulants (e.g., Coumadin, Eliquis, Xarelto)?
BGL (Blood Glucose Level): EMT’s may have a glucometer in thier medical kit and can check their blood sugar. Severe hypoglycemia (low blood sugar) can perfectly mimic a stroke.
AOR Professional GUIDELINES
Stay nearby and re-assess the BE FAST metrics every five minutes as advanced life support is summoned and arriving. Strokes are dynamic; an ischemic stroke can convert into a hemorrhagic stroke right on the sand.
Note if the facial droop or arm drift is progressing, and hand that exact timeline directly to the responding paramedic in charge.
For ocen rescuers and potential stroke victims it’s all about TIME and COMMUNICATION that will help drive a successful outcome. Be ready … and BE FAST.